

Introduction
Despite recent developments on various transplantation procedures and supportive therapy, nonrelapse mortality (NRM) after allogeneic stem cell transplantation (allo-SCT) remains an essential issue. In choosing the appropriate regimen for allo-SCT, decision-making information that considers the complexity of different risk factors is vital. The Hematopoietic Cell Transplantation-Comorbidity Index (HCT-CI), which was initially derived and validated by investigators at the Fred Hutchinson Cancer Research Center to predict NRM, has become a widely validated tool for predicting outcomes in many transplant settings (Sorror et al. Blood. 2005). It can also stratify patients for the risk of other outcomes, including overall survival and graft versus host disease. Patients with a high HCT-CI score tend to prefer allo-SCT with reduced-intensity conditioning. Conversely, for those who prefer allo-SCT with myeloablative conditioning (MAC) and has a low HCT-CI score, a prognostic indicator is unnecessary. Furthermore, the risk factors for NRM may differ among various conditioning regimens. Therefore, the current study aimed to establish a new prognostic model for patients specific to each MAC regimen before allo-SCT.
Methods
We performed a retrospective cohort study to develop prognostic models of NRM in patients conditioned with cyclophosphamide/total body irradiation (Cy/TBI) or busulfan/cyclophosphamide (Bu/Cy). We selected patients who had leukemia and lymphoma in remission or had untreated or stable myelodysplastic syndrome and experienced initial allo-SCT relapse between 2007 and 2017 in the Kanto Study of Group for Cell Therapy (KSGCT). The primary outcome measure was 2-year NRM. Furthermore, we evaluated variables such as patient age, albumin, liver function, renal function, respiratory function, ejection fraction (EF), C-reactive protein (CRP), stem cell source, donor type, antithymocyte globulin use, performance status, recipient/donor sexes, time interval from diagnosis to transplant, and HCT-CI score. To identify a set of variables for Cox proportional hazards, we used an Akaike Information Criterion (AIC)-based variable selection procedure. We assigned weights to individual parameters according to their prognostic significance in Cox proportional hazard models. The identified model's discriminative ability was assessed by Harrell's C-statistic calculated using the bootstrap method.
Results
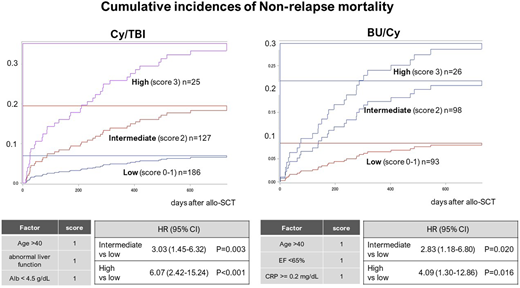
Among the 555 patients analyzed, 338 received Cy/TBI, and 217 received Bu/Cy. In Cy/TBI and Bu/Cy, the median age was 39 (11-60) and 44 (18-62) years, the HCT-CI score ≤ 2 was observed in 82.1% and 87.6%, and 2-year NRM was found in 13.5% and 16.0% of the patients, respectively. Before transplantation, the most dominant parameters in Cy/TBI were abnormal liver function (AST/ALT or bilirubin >upper limit of normal) and albumin value < 4.5g/dL, whereas those in Bu/Cy were age >40 years, EF < 65 %, and CRP ≥ 0.2 mg/dL. Internal validation with bootstrap resampling showed good discrimination, with C-statistic values of 0.70 (95% CI: 0.69-0.71) in Cy/TBI and 0.68 (95% CI: 0.67-0.69) in Bu/Cy. Each of the abovementioned parameters, including age >40 years, was scored as 1 point. To evaluate the 2-year NRM, we divided the total scores into three risk groups. In the Cy/TBI group, the NRM was 6.9% in low (score 0-1, n = 186), 19.5% in intermediate (score 2, n = 127), and 35.3% in high (score 3, n = 25) scores. In the Bu/Cy group, the NRM was 8.3% in low (score 0-1, n = 93), 21.7% in intermediate (score 2, n = 98), and 29.8% in high (score 3, n = 26) scores (Figure). Higher scores were strongly associated with worse NRM and survival.
Conclusions
Our prognostic models for NRM estimation can distinguish patients with a high NRM risk. To our knowledge, these models are the first prognostic models used to estimate NRM for standard-risk patients specific to each MAC regimen. This new simple index may help predict NRM and choose an appropriate conditioning regimen before allo-SCT.
Nakasone:Takeda Pharmaceutical: Honoraria; Otsuka Pharmaceutical: Honoraria; Bristol-Myers Squibb: Honoraria; Celgene: Honoraria; Pfizer: Honoraria; Novartis: Honoraria; Janssen Pharmaceutical: Honoraria; Eisai: Honoraria; Chugai Pharmaceutical: Honoraria; Nippon Shinyaku: Honoraria. Fujisawa:Takeda Pharmaceutical Company Limited.: Speakers Bureau; Astellas Pharma Inc.: Research Funding, Speakers Bureau; Otsuka Pharmaceutical: Speakers Bureau; Pfizer Japan Inc.: Research Funding, Speakers Bureau; Bristol-Myers Squibb Company: Speakers Bureau; Novartis Pharma KK: Research Funding, Speakers Bureau; Celgene: Speakers Bureau; Janssen Pharmaceutical K.K: Speakers Bureau; NIPPON SHINYAKU CO.,LTD.: Research Funding. Nakaseko:Novartis Pharma KK: Speakers Bureau; Pfizer Japan Inc.: Speakers Bureau. Kanda:Novartis: Honoraria; Kyowa Kirin: Honoraria, Research Funding; Bristol-Myers Squibb: Honoraria; Takeda Pharmaceuticals: Honoraria; Alexion Pharmaceuticals: Honoraria; Shire: Honoraria; Daiichi Sankyo: Honoraria; Ono Pharmaceutical: Honoraria; Nippon Shinyaku: Honoraria, Research Funding; Mochida Pharmaceutical: Honoraria; Mundipharma: Honoraria; Sanofi: Honoraria, Research Funding; Meiji Seika Kaisha: Honoraria; Shionogi: Research Funding; Otsuka: Honoraria, Research Funding; Celgene: Honoraria; Chugai Pharma: Honoraria, Research Funding; Eisai: Honoraria, Research Funding; Janssen: Honoraria; Astellas Pharma: Honoraria, Research Funding; Sumitomo Dainippon Pharma: Honoraria; Pfizer: Honoraria, Research Funding; Merck Sharp & Dohme: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal